Identification of Medical Personnel, Vehicles and Installations
View of an Aid Station run by medical personnel belonging to the 10th Mountain Division, Italy, April 1945
Background Information:
It was important to clearly identify Medical personnel in the field. One of the early documents, such as the “Amelioration of the Conditions of the Wounded in Armies in the Field” signed August 22, 1864, by a number of Governments, already instructed that Flag and Arm Badges worn by Medical personnel would bear a Red Cross on a White Field. Both symbols when used on Hospitals, Ambulances, Evacuation and Aid Centers, were to be proof of their neutral status! These signs provided for neutrality of military and civilian protected personnel (it gave them non-belligerent status) exclusively engaged in removal, transportation, and treatment of wounded and sick, or the administration of sanitary formations and establishments, and entitled them to respect and protection from their enemies. The “1929 Geneva Convention” which superseded the former agreement, was signed on July 27, 1929 by forty-seven countries (including the Axis countries, Germany, Italy, and Japan) and comprised numerous articles, among which Articles 9 and 21, recognizing that bearers of special identification cards and civilian protected personnel identified by armbands, and vehicles, and installations wearing Geneva Convention markings and markers, were all exclusively engaged in medical care activities, and consequently protected and respected by the Geneva Convention.

Jeep Ambulance pertaining to the Medical Detachment of the 32d Armored Regiment (3d Armored Division), note extra Geneva Convention markings
The term Geneva Convention, derived from the Convention itself, applied to a number of documents and items of identification and/or recognition, used by Medical personnel while active in the field. We will discuss a number of ‘official’ items, as well as non-official means initiated to enhance identification and recognition of medical personnel, medical vehicles, and medical installations.
Medical Department Geneva Convention Identification Card:
The Geneva Convention I.D. Card, first pattern, introduced in 1942, was distributed to medical personnel in accordance with instructions of the “1929 Geneva Convention” (requiring that medical and civilian protected personnel should wear the necessary ID in order to be recognized as non-belligerents). The document looks very similar to the existing War Department I.D. Document in use during WW2; this was however a threefold document, whereas the Geneva Convention document was only a twofold document!
First pattern Geneva Convention ID Document, bearer Edgar L. DOUTY, ASN 33164775, Tec 5, Medical Department, US Army
The front cover is medium brown with black markings, stating UNITED STATES OF AMERICA, WAR DEPARTMENT, Coat of Arms, MEDICAL DEPARTMENT, RED CROSS, Identification Card, except for the No.+ sequence of digits, which are red. The back cover, bears a special text, i.e. Loss of this card will be reported through channels to the Force Commander without delay., followed by a printed Red Cross and another short text, Issued in accordance with Article 21, Geneva Treaty, July 27, 1929., with signature, and indication, Major General, The Adjutant General of the Army., and, W.D., A.G.O. Form No. 65-10, May 20, 1942, GPO 16-25005-1. The double page inside folds in the middle, and contains headings to be filled out, such as; THIS IS TO IDENTIFY– Agency, First Name, Middle Name, Last Name, Race, Birth Date, Color Eyes, Height, Signature of Bearer, Military Authorization-Signature, Date, Place – the rest of the page is reserved for Fingerprints (Right Hand, Thumb, Index and Middle Finger), a B/W picture of the card bearer and reference 16-28605-1.
Second pattern Geneva Convention ID Card (laminated), bearer Jennings D. BANNER, ASN 17000575, Sgt, Medical Department, US Army
A new and improved Geneva Convention I.D. Card followed, this is the second pattern version (laminated). It was introduced later in the war and was not only easier to carry and handle, moreover it was coated with transparent plastic for enhanced protection. The document obverse side is an ivory-white rectangular card with a red frame, red headings and indications e.g. the frame itself bears following statement, NOT A PASS – FOR IDENTIFICATION ONLY, PROPERTY OF U.S. GOV’T., LOSS OF THIS CARD MUST BE REPORTED AT ONCE and further WAR DEPARTMENT, THE ADJUTANT GENERAL’S OFFICE, WASHINGTON, D.C., followed by the US War Office Coat of Arms and CERTIFICATE OF IDENTITY TO BE ISSUED TO MILITARY AND CIVILIAN PROTECTED PERSONNEL, with indication of Name, Designation, Signature, Date Issued, Countersignee, and reference W.D. A.G.O. 65-10. It also holds sufficient space for a black and white picture of the card holder. The reverse side has following indications in black; Height, Weight, Hair, Eyes, Date of Birth, Fingerprints, Left Index, Right Index, Identification No., with sufficient space, while the larger part (right) is covered by a red cross over which a black text is superimposed defining the duties of the card bearer, as well as a note related to possible loss of the card and a public warning. The number of digits preceded by a block letter, is supposedly the same one as stamped on the inside of the medical brassard, authorized by the Geneva Convention.
It is estimated that approximately 830,000 cards were distributed to medical personnel in the course of WW2. After the war, a new (smaller) Geneva Convention Identification Card was issued by the US Government bearing reference to the following Geneva Convention, which took place August 12, 1949.
Geneva Convention Brassard (item #9913500):
Obverse and reverse views of the M-1924 Geneva Convention Brassard, note the extra texts on the reverse side
In order to comply with the Geneva Convention and Army Regulations a Medical Brassard was introduced November 25, 1924 for general wear by all medical personnel active in the field. As was the case with other armbands, this one was also to be worn on the left sleeve, above the elbow. It represented a red percale cross (3 inches x 3 inches) stitched on a white rectangular cotton (4 inches x 18 inches) armband, which was fixed to the clothing by a large safety pin. Every official brassard had a black ink stamped text on the inside stating “issued by Medical Department, U.S. Army, in conformity with Article 21, International Red Cross Convention, Geneva, 1929” – furthermore there was another stamped text showing the Identity Card number (of the holder) i.e. a black block letter, followed by a number of digits. This number was also reflected on the Medic’s Geneva Convention Identification Card, which he had to carry with him at all times, in order to remain protected as a non-combatant or neutral member of the Armed Forces by the terms of the Geneva Convention applicable in time of war. A similar means of identification (item #9913700) was introduced for the Veterinary Corps December 13, 1939; it carried a green cross on a white rectangular field, but its members were however not protected by the Geneva Convention.
On 16 June 1944, it was confirmed by the Chaplain Section, Headquarters, Communications Zone, ETOUSA, that Chaplains and Chaplains’ Assistants, Enlisted Men and Warrant Officers, who were concerned exclusively with the removal, transportation, and treatment of the sick and wounded, were permitted to wear the Medical Department GC Red Cross brassard.
Detailed view of ID Card Number with prefix Letter, stamped onto the reverse side of the Geneva Convention Brassard
Detailed view of the official text stamped by the Medical Department on the reverse side of the Geneva Convention Brassard
Another detailed view of the official text (different style) stamped by the Medical Department on the reverse side of the Geneva Convention Brassard
Geneva Convention Helmet:

Geneva Convention Brassard being tucked behind camouflage net of Steel Helmet, field improvisation
Although widely spread throughout World War 2, the use of Geneva Convention helmet markings was never official – indeed there were no Army Regulations governing their use!

Variations in Geneva Convention Symbols Helmet Markings (reproductions)
Apparently, the first use of medical markings on steel helmets took place in N. Africa (NATOUSA Theater) around mid-1943. During “Operation Torch” (Invasion of North Africa, 8 Nov 42) and subsequent field activities, it had been noted that quite a lot of medical aid men suffered regular casualties. Interrogation of German PWs revealed that the single Red Cross brassard (worn on the left arm) was not always visible, during combat, and as such it was often difficult for the enemy to correctly identify medics in the field! An investigation was launched and upon instructions from The Surgeon General’s Office, reports from the N. African & Mediterranean Campaigns were intensively studied. It took a while to remedy the situation, and meanwhile medical personnel (1943-44) just placed a second brassard under the helmet’s camouflage net in order to show their trade more distinctively. Some men began to wear a brassard on both arms for increased identification (left and right). Finally, in the end, medics just started painting red cross symbols directly onto the helmet itself. This use was gradually introduced in the Italian Theater, and later expanded to the ETOUSA, after the Normandy landings. It seemed that the Medical Department was afraid of the enemy’s reaction, for the coming D-Day Operation (6 Jun 1944), whereby medics refrained from painting any Red Cross markings on their helmets – this can be clearly seen in period illustrations (though, with minor exceptions)! When the Allies moved further inland, they seemed appeased. After 2 months of combat and careful analysis of shooting accidents, involving medical personnel, in Normandy, most unit commanders concluded that, except for isolated cases, the Germans abided by the Geneva Convention. According to statements made by German prisoners, sniper incidents often resulted from difficulty in seeing and identifying Geneva Convention brassards on men moving in the field, furthermore American medics in some Divisions noted that a high proportion of their small-arms casualties were often shot from the unbrassarded right side! Some aidmen and litter bearers accordingly began to wear brassards on both arms, and even started painting non-regulation red crosses on their steel helmets (just as happened in the Mediterranean Theater). The XIX Corps Surgeon late in July 1944 officially authorized these painted markings and other measures to make Geneva Convention symbols on men and vehicles more conspicuous.

Medic helping an injured man, Geneva Convention Red Cross painted on Whitewashed Steel Helmet, winter improvisation
In certain units, the Chief Surgeon defined the kind of marking that was supposed to adorn the medic’s helmet, while in other units, there was no specific standard to adhere to – this explains the widespread variety in helmet markings (sofar we discovered over 20 different markings, in period-photographs), whereby colors, dimensions, combinations and even the red cross symbol differ a lot … sometimes stencils were used, but the majority were merely handpainted markings… the most widely used symbol was a red cross on a white circular field (identical to the Geneva Convention brassard). Change N°5 to AR 850-5 dated 15 February 1945 was only introduced on January 23, 1948 to regulate official use of a red Geneva Cross on a white circular background for medical personnel helmets – it was however shortlived, since already cancelled on 18 January 1949 by Change N°6 (due to the introduction of helmet covers, which made any markings redundant).

Variations in Geneva Convention Symbols painted on Steel Helmets
Medical Tabards:

Medics from the 94th Infantry Division trying on Geneva Convention Tabards, all Aid Men are wearing Brassards on both arms, also note the different sizes of Helmet Markings
White Tabards or Aprons with Red Crosses (worn over breast and back) were apparently first introduced in February 1945. This kind of garment was based on German models, and was supposed to enhance visibility and identification of Medical personnel in combat and field conditions. Third United States Army (Lt. General George S. Patton’s outfit) claims to have introduced this additional means of identification.
Geneva Convention Flags and Markers:
In accordance with Geneva Convention recommendations and instructions, the War Department introduced a number of Flags and Markers for identification of medical installations and vehicles.
Flag, Ambulance and Marker, Stock No. 5-F-2150:
Primarily used to distinguish Ambulances and Aid Stations protected by the Geneva Convention. The flag or marker consisted of 12-inch Red Cross centered on a White rectangular Field 18 by 27 inches. The flag (when not in use) could be covered by a Case, Flag, Duck, Automobile, Stock No. 5-C-50, the staff was officially designated Flagstaff, Wood, Marker and Marker Pennant, Stock No. 5-F-6590.

Ambulance Flag and Marker, traditional Red Cross centered on a White rectangular Field (flagstaff missing)
Flag, Field Hospital, Stock No. 5-F-2160:
Used for identification of mobile Hospitals, primarily Field Hospitals. The flag had following characteristics; a 36-inch Red Cross on a White rectangular Field, 48 inches by 72 inches.
Flag, General Hospital, Stock No. 5-F-2170:
Used for identification of fixed and semi-mobile Hospitals (i.e. General Hospitals). Description; a 54-inch Red Cross on a White rectangular Field, 72 inches by 108 inches.
Needless to add, that improvised field solutions were also used, such as locally-made Flags.

Aerial view of a Field Hospital, note the Red Cross Canvas Marker in the foreground left, and the circular Red Cross Markers displayed over the different Hospital Wards
Markers were more generally used to enhance aerial recognition and identification by either friend or foe.
Marker, Red Cross, Canvas, Stock No. 5-M-300:
Introduced to distinguish individual tentage used for medical purposes. The Markers were placed over the ridge of the tent with one half of its length displayed on either side. This method allowed for a clear and distinguishable Geneva Red Cross on both sides of the tent’s roof. Primarily used on Hospital Wards and Surgical Tents.
Marker, Red Cross, Canvas, Stock No. 5-M-3050:
Introduced to facilitate aerial identification from altitudes up to and including 20,000 feet on clear days. These Markers were used on the ground to designate Hospital areas and were designed for easy, quick assembly, anchoring and dismantling. The individual sections were provided with covers for protection against soiling.
Miscellaneous Geneva Convention Symbols:

Extra Geneva Convention Cover draped over a 1/4-Ton Vehicle’s hood
(re-enactment)
Although never official, miscellaneous or add-on medical symbols were used to underline the medical nature of the vehicle and organization, and they did help. Vehicle drivers often replaced the white star on the hood by a painted Red Cross on a White Field. The windshield cover was also sometimes adorned with Geneva Convention markings (instead of a star). In other instances, a Red Cross on a White Field, was sometimes draped as a cover over the vehicle’s bonnet, or attached to the canvas of trucks used by the Medical Department.
A 3/4-Ton Weapons Carrier serving as makeshift Ambulance, crossing ‘Siegfried Line’ (Westwall) Dragon Teeth antitank defense elements

Add-on and painted Geneva Convention Symbols on Truck canvas tarpaulin and Blood Refrigeration Unit
Medical Dog Tags:
Brass Identification Tag, holder Flora A. PERCIVAL, N 743921, 2d Lieutenant, Army Nurse Corps, US Army
A few Identification Tags displayed special prefixes related to medical specialties. Following Dog Tags were introduced in the course of WW2 :
Army Nurse Corps (ANC-established 1901) – prefix N, followed by a series of digits designating the individual Army Serial Number.
Hospital Dietitian (HD-established 1942) – prefix R, followed by a series of digits designating the individual Army Serial Number.
Physical Therapist (PT-established 1942) – prefix M, followed by a series of digits designating the individual Army Serial Number.
Contract Surgeon (CS-established 1941) – prefix CS, followed by a series of digits designating the individual Army Serial Number.
For general information, American Red Cross (ARC) volunteers (not Army personnel), were issued special Dog Tags, with following embossed data; prefix ARC, followed by a series of digits designating the bearer’s individual Serial Number.
A ‘special’ Tag was made by the Graves Registration Service (GRS), when it proved impossible to determine the identification of an unknown soldier and personal Dog Tags were missing. The bodies were marked – unknown – and a substitute Identification Tag was then embossed with following indication; UNKNOWN SOLDIER, X-5102, GRS. (X was the designation for ‘unknown’, while the series of digits, was just the next numeral, assigned to the remains of an unknown soldier being buried in a temporary cemetery).

Stainless Steel Substitute Dog Tag for an Unknown Soldier (Known but to God), with ‘special’ Serial Number provided by the Graves Registration Service (QMC)
Medical Guidon:
Illustration of a Medical Guidon, this one belongs to “Dog” Company, 26th Medical Training Battalion, Medical Replacement Training Center, Cp. Grant, Illinois, June 1943 (note the Guidon does not have the M, it only displays RTC)
Official unit identification flag or marker approved by the War Department. General dimensions were as follows; 20 inches hoist by 2 feet ¾-inch fly, swallow tail end forked-10 inches. The swallow-tailed Guidon used the colors of the branch it represented, in this particular case, Maroon and White, and the service insignia as well, i.e. the Caduceus, it had no fringe. Guidons were made of wool bunting cloth. They were usually carried by units participating in parades, reviews, and special ceremonies, or displayed as directed by the organization’s Commanding Officer. Streamers could be awarded and thereby became intrinsic components parts of the Guidon, they were attached below the spearhead of the flagstaff. Every Guidon was provided with a canvas cover, i.e. Case, Guidon, Stock No. 5-C-65.

Left: Guidon, Medical Detachment, 116th Infantry Regiment, 29th Infantry Division (Campaign credits; Normandy, Northern France, Rhineland, Central Europe).
Right: Guidon, Medical Detachment, 395th Infantry Regiment, 99th Infantry Division (Campaign credits: Rhineland, Ardennes-Alsace, Central Europe).
Medical Badge:
The Medical Badge was only introduced on March 3, 1945 for medical personnel who served with the Medical Detachments of Infantry units during WW2. Introduction of both E.I.B. (Expert Infantryman Badge) and C.I.B. (Combat Infantryman Badge) in November 1943 created an administrative problem and caused wide concern about medical personnel and infantrymen. Although medical personnel, regularly attached to Army Infantry Regiments and/or Battalions were running considerable hazards when carrying out their duty, they were NOT entitled to the C.I.B.! (though some Commanders did obtain CIBs for the combat medics). Army Regulations strictly forbade granting combat awards, since this was against the Geneva Convention and the non-combatant (i.e. neutral) status of medical personnel! In fall of 1944, the War Department once more stressed that it was forbidden to grant EIBs and CIBs to medical personnel and Chaplains! This was because a lot of Infantrymen (acknowledging the risk and courage of attached medical personnel) complained that it was unfair to treat aidmen this way, and also some people were thoroughly frustrated they could not earn the extra $10.00/month of combat pay (which came with the CIB award). Hence the introduction by the Surgeon General’s Office of a special badge to honor medical personnel! The design was only adopted 3 March 1945, and the official uniform regulations appeared on April 18, 1945 (C-3 of AR 600-35).

Medical Badge, created and authorized by the War Department on March 1, 1945 for personnel serving with Medical Detachments of Infantry Regiments (or smaller units), in fact a ‘companion’ Badge to the CIB (Combat Infantryman Badge) specifically intended for medical personnel
Description:
(AG 421/3 Mar 45) “A STRETCHER PLACED HORIZONTALLY BEHIND A CADUCEUS WITH THE CROSS OF THE GENEVA CONVENTION AT THE JUNCTION OF THE WINGS, ALL ENCLOSED BY AN ELLIPTICAL OAK WREATH 1-IN IN HEIGHT AND 1 ½ -IN IN WIDTH, OF OXIDIZED SILVER”. Official statement: The War Department has authorized wear of a Medic’s Badge for personnel who served with the Medical Detachments of Infantry Regiments or smaller units, since the beginning of the War. The subsequent Bill of Congress will give those people an extra $10.00-a-month pay as provided for combat infantrymen. Medics up to and including rank of Captain are eligible, as well as Regimental Surgeons. The Medical Badge shall be worn above decorations and/or ribbons, over the left breast pocket of the uniform coat or jacket.
Insignia:
Army Regulations 600-40 prescribed a number of Insignia for wear on uniform clothing. These Insignia destined for wear on collars and lapels were made of gold-colored metal. Attachments consisted of screw backs, safety pins, or clutches. Insignia for Officers were different from those worn by Enlisted Men.
Uniform Insignia:
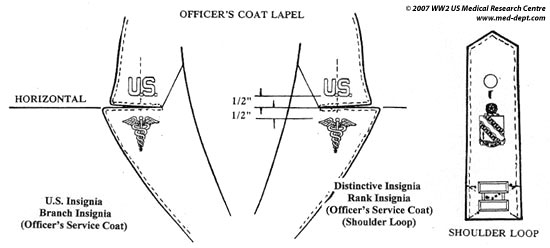
Figure illustrating location of U.S. and Branch of Service Insignia on Service Coat + D.I. and Rank Insignia on Shoulder Loops

Figure illustrating location of Rank and Branch Insignia on Shirt Collar
Officers:
U.S. – Officers will wear block letters U.S. 7/16 inch in height, each letter to be followed by a period symbol. Insignia will be worn on both upper lapels of the Officers’ Coat.
Insignia of Arm or Service – Officers pertaining to the Medical Department will wear the appropriate Caduceus device, 1 inch in height, and if letters are used, they will be 3/8 inch in height. Service Insignia will be worn on both Coat lapels (under both U.S. letters), or on the left Shirt collar (when no Service Coat is worn). Elements superimposed on Officers’ Insignia will be of bronze finish or brown enamel (for illustrations of the different medical branch insignia, kindly revert to our article “Brief Overview of the Medical Department”).
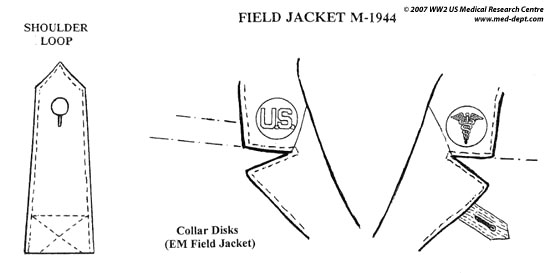
Figure illustrating location of Collar Disks on Field (IKE) Jacket
Enlisted Men:
U.S. – Enlisted Men will wear the letters U.S. on a plain solid circular background or disk, 1 inch in diameter, on the right collar lapel of the Service Coat. Material used is thin brass stamping, but it is to be noted, that due to temporary metal shortages, plastic disks were also manufactured and used.
Insignia of Arm or Service – Enlisted personnel of the Medical Department will wear the appropriate Caduceus symbol on a similar plain circular background or disk, on the left Coat collar lapel.
Headgear Ornamentation:
Officers:
Officers will wear a cord edge braid of gold bullion (or metallized cellophane) and black silk intermixed. (for Warrant Officers, color will be silver & black, for General Officers, color will be overall gold, for Chaplains, color will be identical to Officers, although some Chaplains continued to use the black braid worn during WW1).

Illustration of Medical Piping (Maroon/White) and DI (61st Medical Battalion / 5th Engineer Special Brigade, campaigns: Normandy, Northern France, DI: approved 13 Jan 43) on Garrison Cap
Enlisted Men:
Enlisted personnel will wear a cord edge braid (or piping) corresponding to the Arm or Service , for the Medical Department it is Maroon piped with White. As there were periods of war shortages, and difficulties in overseas transportation and supply, Garrison or Overseas Caps worn in the E.T.O. were not always adorned with the appropriate piping.
Service Coat & Headdress Distinctive Insignia:

Illustration of Collar Disks, as worn on Class A Uniforms
Each Regiment and independent Battalion of the United States Army was authorized a Coat of Arms (for display on its organizational flag) and a Distinctive Insignia (D.I.) for wear on the uniform. The Coat of Arms is a heraldic representation embroidered in the branch colors, representing the unit’s history, tradition, ideals, and accomplishments, and serves as an inspiration and an incentive for unity of purpose. The Distinctive Insignia is based on all, or some elements of the Coat of Arms, and is usually made in the Arm or Service basic colors. It is worn on the uniform to promote ‘esprit de corps’. The practice was temporarily dropped, when the WD announced in January 1943 that no further D.I.s would be approved or manufactured for the duration of the war. If adopted, D.I.s must be worn by the entire personnel of the organization. It should be noted that Distinctive Insignia had to be duly approved and authorized, before the unit was allowed to wear them!

Figure illustrating location of Piping and Distinctive insignia on Garrison (Overseas) Cap
Officers:
Officers will wear the unit’s specific (approved) Distinctive Insignia centered on both Shoulder Loops of the Service Coat (or centered on the Green Leader loops). Since Officers were wearing their Insignia of Grade on the left side of the Garrison Cap, there was no room left for D.I.s.
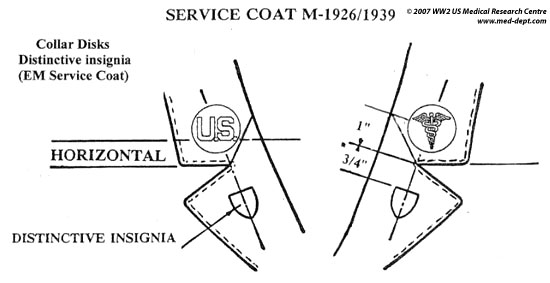
Figure illustrating location of Collar Disks and D.I.s on Service Coat
Enlisted Men:
Enlisted personnel will wear the D.I.s on both sides of the Lapels of the Service Coat, ¾ inch below the lapel notch . They will also wear it on the left side of the Garrison Cap, 1 ½ inches to the left of the front center part.

Samples of Distinctive Insignia – from L to R:56th General Hospital (campaigns: Normandy, Northern France, Rhineland, DI: approved 15 Jan 42)
24th Medical Battalion / 24th Infantry Division (campaigns: Central Pacific, New Guinea, Leyte, Luzon, Southern Philippines, DI: approved 29 Sep 23)
12th Field Hospital (campaigns: Normandy, Northern France, Rhineland, Central Europe, DI: approved 19 Jan 43)
9th Medical Battalion / 9th Infantry Division (campaigns: Algeria, French-Morocco, Tunisia, Sicily, Normandy, Northern France, Rhineland, Ardennes-Alsace, Central Europe, DI: approved 12 Mar 41)
21st Evacuation Hospital (campaigns: Sicily, Naples-Foggia, Rome-Arno, Southern France, Rhineland, Ardennes-Alsace, Central Europe, DI: approved 8 Dec 42)
Remark
Service Hats (or Campaign Hats) have not been included, for obvious reasons. The above Regulations only reflect wear of insignia and trimmings in the E.T.O., i.e. after 1942.
Technicians:
Chevrons for Noncommissionned Officers and Privates First Class, including the new Technicians introduced in 1942
The system of Army Specialist Ratings (6 Classes) was discontinued and a new system was to be put into effect, granting NCO rank to ‘Specialists’ (Enlisted Men doing work that required ‘specialized’ training). Following grades were added by War Department Circular No. 5, dated January 8, 1942: they were respectively Technician Third grade, Technician Fourth Grade,and Technician Fifth Grade – the corresponding Chevrons were to receive an additional symbol, the letter “T” for Technician, introduced by War Department Change C-1, Army Regulations 600-35, dated September 4, 1942.
Tec 3, Tec 4, and Tec 5 were to rank immediately below Staff Sergeant, Sergeant, and Corporal. Technicians thus became ‘Noncommissioned Officers’, and received pay, allowance, and privileges of the pay grade specified by their title. Although the new Technicians achieved NCO status, they were forbidden to exercise any tactical control in the field!
Among the wide range of medical ‘Specialists’ were: Veterinary Technicians, X-Ray Technicians, Medical Technicians, Dental Technicians, Medical Laboratory Technicians, Pharmacy Technicians, Surgical Technicians, Sanitary Technicians, and Equipment Maintenance Technicians.