WW2 Military Hospitals General Introduction

Valley Forge General Hospital, at Phoenixville, Pa., one of the ‘named’ Hospitals. Designated US Army Gen Hosp by WDGO 64, dated 24 Nov 42. The construction consisted of a two-story high semi-permanent brick building, with an authorized bed capacity of 2,509. First patients were received as from 12 Mar 43. Medical specialties were plastic surgery, ophthalmologic surgery, and blind psychiatry.
Background Information:
In time of war Hospitalization and Evacuation are essential to the Armed Forces. Military Hospitals are provided for the treatment of military personnel while being sick or injured. Casualties were given emergency treatment at a series of medical installations established in the forward areas of combat zones. In order to furnish as near to the front lines as possible, a higher type of medical treatment than first aid or emergency medical care, Hospitals, either ‘fixed’ or designed for easy movement, i.e. ‘mobile’ (or semi-mobile) Hospitals were established. Mobile Hospitals, such as Surgical, Evacuation, and Convalescent Hospitals were usually assigned to field Divisions and Armies. All Hospitals in Theaters of Operations (i.e. overseas) were designated by numbers rather than by name and location (limited to ZI).
In war, ‘mobile’ Hospitals formed a constituent part of the mobile forces and were equipped with sufficient tentage for sheltering patients; nevertheless, advantage was taken of any opportunity to occupy and utilize existing buildings. These Hospitals were established in the combat zone and comprised Convalescent Hospitals, Evacuation Hospitals, Surgical Hospitals, but also Clearing Stations operated by the Clearing Companies of Medical Battalions. The ‘fixed’ military Hospitals, identical in time of war or peace, served for definitive treatment of patients. They were established in the Zone of Interior and in the Communications Zones. Those set up in the Communications Zones (ComZ) included General Hospitals, Station Hospitals, Hospital Centers, Convalescent Camps and Centers, and Field Hospitals. Whenever practicable, three or more General Hospitals were grouped at one place into a single administrative and clinical organization known as a Hospital Center (usually with an attached Convalescent Camp).
Numbers of Hospitals in Operation at the End of World War Two:
On 8 May 1945, at the close of hostilities in the different Theaters of Operations, United States Army Forces (including the Army Air Forces) were deployed as follows:
European Theater of Operations
The total strength represented 3,065,505 men; these troops were served by a total of 290 Hospitals, including 34 Field Hospitals – 47 Station Hospitals – 63 Evacuation Hospitals – and 146 General Hospitals.
Mediterranean Theater of Operations
The total strength of the Armed Forces was 493,876 men; these were medically supported by a total of 47 Hospitals, including 7 Field Hospitals – 8 Evacuation Hospitals – 11 General Hospitals – and 21 Station Hospitals.
Pacific Theater of Operations
By 15 August 1945 a total of 1,389,010 troops were deployed in the different areas; these were served by a total of 146 Hospitals, including 15 Evacuation Hospitals – 24 Field Hospitals – 46 General Hospitals – and 61 Station Hospitals.
Types of Hospitals:
Convalescent Camps were located in the vicinity of and were part of the Hospital Centers. They relieved the General Hospitals of the necessity for caring for patients who no longer required hospital treatment, but who were not yet fit for duty. In practice, such camps were equipped to accommodate 20% of the total capacity of the Hospital to which they belonged.
Convalescent Hospitals were included in the organization of a type Army. They were designed to care for cases who would probably fully recover and be ready for duty within the limit set by the Theater Surgeon (120 to 180 days), and who required little or no medical treatment other than observation and rehabilitation. The Hospital received its patients from the Evacuation Hospitals and Clearing Stations, and subsequently transferred them to a Replacement Center or returned them to an Evacuation Hospital. Normal capacity was 3,000 patients, but if necessary, installations could be expanded to accommodate 5,000 patients for a short period.
Evacuation Hospitals were mobile units designed to provide, near the front, facilities for major medical and surgical treatment of casualties, received from Division, Corps, and Army Clearing Stations. Their task was to combine and concentrate the evacuees in such numbers and at such location that mass evacuation by common carrier could be undertaken economically. They also provided the opportunity and facilities for the beginning of a definitive treatment, the sorting of casualties, the return of those men soon fit for duty, and for extended evacuation of certain patients to General Hospitals at some distance to the rear. Patients were supposed to be retained in the hospital from a few hours to a few weeks depending on the rate of admission, necessity for movement, available bed-capacity, and the overall tactical situation. Evacuation Hospitals were of two types: 400-bed semi-mobile and 750-bed mobile.
Field Hospitals were another type of medical installation. They were the last and largest divisional unit of the Medical Department in the chain of evacuation. Such Hospitals received casualties from the dressing station, and utilized all measures possible, under varying conditions, to best fit them for continued evacuation, usually to Evacuation Hospitals. Field Hospitals were usually located from 3 to 8 miles from the front line, depending upon such factors as the enemy range of fire, the roads, the fuel, the water, the presence of buildings, and the location of Evacuation Hospitals. Whenever possible, they were grouped in a village or at the confluence of roads from the sector served, for convenience both in the interchange of patients and for the ambulances. Distinctive features were their mobility and ability to operate three separate Hospital units (or Platoons), if necessary, at widely separated places. When operating separately, these Platoons each formed a complete small hospital.
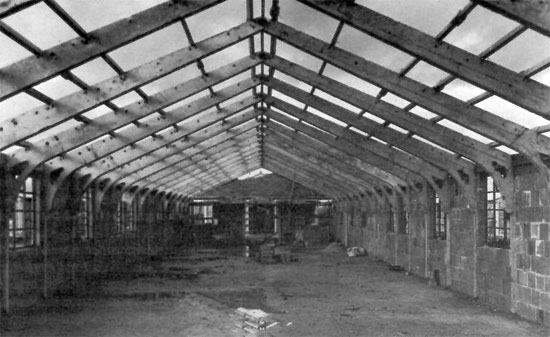
Hospital Construction, somewhere in the ZI, 1943. Solid construction methods employed prefabricated concrete roof trusses. Major projects always involved Corps of Engineers personnel.
General Hospitals were standard establishments with a normal capacity of 1,000 patients (with expansion possibilities in case of emergency to 1,500 or 2,000) equipped to give definitive medical and surgical treatment to all cases. Once located, a General Hospital usually remained in that place throughout the period of operations (depending on the evolution of field and combat operations). These numbered Hospitals received their patients from Evacuation Hospitals located in the combat zone, who arrived by train, ambulance, or airplane. General Hospitals performed the most difficult and specialized procedures, and therefore had the most elaborate equipment in the Theater of Operations.
Hospital Centers were particularly advantageous because they permitted economy in MD personnel, simplified supply and evacuation problems and facilitated overall administration. These Centers consisted of a Headquarters and Service Company, a Central Laboratory, a Convalescent Camp, and a number of General Hospital units assigned to the group, all housed in permanent or temporary buildings or floored (concrete) tents with adequate sewage, water, and electrical facilities.
Station Hospitals rendered general medical and surgical treatment for those areas where there were sufficient military populations to justify their maintenance, but not sufficient to justify General Hospitals. They were usually located at most Posts, Camps, and Stations for hospitalization of local personnel. In the Zone of Interior, such Hospitals were housed in buildings and received names, while in the Communications Zone, they were set up in tentage or improvised housing, and here they were numbered. Bed capacities varied from 25 to 900.
Surgical Hospitals were mobile units designed primarily to furnish, as far forward as practicable, facilities for major surgical procedures for a limited number of serious injury cases, and to relieve Clearing Stations of non-transportable casualties. They even served as a substitute for Evacuation Hospitals in cases of emergency. Their operating teams were often used to reinforce other medical units.
Miscellaneous Hospitals
All-Black Hospitals:
Since the Surgeon General was opposed to integration of African-American doctors and nurses with white professionals (general Government and War Department policy during WW2 –ed), there was no other option but to establish all-black wards in some hospitals, such as Ft. Bragg, North Carolina and Cp. Livingston, Louisiana. These medical installations would only care for African-American patients. The Medical Department mostly employed its limited complement of African-American staff in the black wards of white Station Hospitals, while the majority of black personnel either served in Ambulance and Sanitary Companies, or in the Medical Detachments attached to segregated combat and support units!
In 1942, two all-Black Hospitals were operating, one at Ft. Huachuca, Arizona, run by the Army, and another at Tuskegee, Alabama, run by the Air Corps. Nevertheless, in view of the need for more medical personnel, African-Americans were to serve in other hospitals too. Under pressure from groups and associations advocating more use of black manpower, Army Service Forces Headquarters directed the Surgeon General to procure additional African-American personnel. From there on, such medical personnel were used on a non-segregated basis in 4 General Hospitals, 3 Regional Hospitals, and 9 Station Hospitals in the ZI, be it still under white command! Overseas, the 335th Station Hospital (CBI), the 268th Station Hospital (SWP), the 355th and 383d Station Hospitals (CBI and Philippines), and the 25th Station Hospital (Liberia), as well as the 168th Station Hospital (England) had their complement of Black nurses. By the end of 1944, the Medical Department employed 342 African-American Officers and 19,587 Enlisted Men and Women.
Army Hospitals for Civilians:
Towards the end of 1942, when the Ordnance Department established Storage Depots of explosives in isolated places, the overall lack of hospitals or sufficient medical facilities retarded civilian employee procurement and also increased absenteeism of the labor force! The failure to provide prompt medical care and treatment often resulted in prolonged illness. In February 1943, the Secretary of War, upon proposal of the Surgeon General, decided to finance construction of 6 Army Hospitals, under Service Command supervision, with a minimum of military personnel, in order to provide family medical care, additional gynaecologic and obstetric services, and requiring payment for services rendered. The system proved successful!

Aerial view of Ft. Davis and Station Hospital (in fact no more than a Dispensary), in the Panama Canal Zone, 1942. Before WW2 (1940), the Department operated 6 small Hospitals and 4 Dispensaries, which provided the necessary medical service. The very first permanent Army Hospitals only opened in September 1943 – in total only 3 new Hospitals were ever built, and temporary installations had to tackle any peak loads of patients.
Prisoner of War Hospitals:
Based on the Geneva Convention, basic policies for medical treatment of enemy PWs were jointly discussed and set up by the Provost Marshal General and the Surgeon General. Hospital accommodations and medical care for Prisoners of War were to be equal to those offered to United States troops, and enemy medical personnel or PW volunteers were invited to assist in the care of their fellow compatriots. For separate PW Camps in the ZI, the Army constructed Hospitals with beds for 4% of the inmates. For PWs held at Army Posts, hospital wards were to be surrounded by barbed wire fences. Such Prisoner of War Hospitals operated under Service Command supervision, and were very much similar to other Service Command Hospitals, except for the use of captured enemy medical personnel, and the use of enhanced security measures.
Following capture by American Forces of large numbers of German and Italian prisoners, those who became sick or were injured while interned in the Zone of Interior, were treated at Station Hospitals located either in the particular Internment Camps or on nearby Army Posts or Camps, and if in need of a higher type of care in General Hospitals operated for US Army patients. For the Japanese PWs, the solution was simple. Since they were few in numbers, all were sent to the Station Hospital, Camp McCoy, Sparta, Wisconsin.

Aerial view of Camp McCoy, Sparta, Wisconsin, the largest holding facility for Japanese Prisoners of War in the Zone of Interior (this camp housed both relocated Japanese-Americans from the West Coast, as well as German, Italian, and Japanese PWs captured during WW2).
Procedures for the reception – examination – and transportation of enemy patients had already been established by both the Offices of The Surgeon General and The Provost Marshal General in April 1942, and reiterated in September 1943, and were to govern the general policy for the hospitalization of enemy Prisoners of War throughout the war period. A total of five (5) General Hospitals located near Debarkation Ports had been selected. Although it was foreseen to concentrate those prisoner patients received from Theaters of Operations overseas as well as those transferred from Internment Camps in the ZI, in ONE General Hospital if possible, and in not more than three (3) in any instance, in each Service Command, this did not always prove possible. Dispersal made the work of the Commission (responsible for Hospitalization, Evacuation, and Disposition of PW Patients) difficult and determining the eligibility of some Prisoners of War for possible repatriation as well as certifying others for “protected status” as medical personnel under the Terms of the Geneva Convention, remained a problem.
In July 1944 (following D-Day operations in the ETO) it was proposed to devote at least ONE General Hospital exclusively to German PWs. In anticipation of a large influx of prisoner patients after the Invasion of Europe, The Surgeon General, and ASF Headquarters, suggested the designation of additional PW General Hospitals.
On 21 July 1944, Glennan General Hospital (Okmulgee, Oklahoma, opened for patients 17 Dec 43, bed capacity 1,690, disposed of last patient 2 Dec 45) was designated German Prisoner of War General Hospital No. 1. Early October 1944, the Station Hospital at Camp Forrest (Tullahoma, Tennessee, opened for patients 21 Oct 44, bed capacity 2,500, disposed of last patient 15 Dec 45) became Prisoner of War General Hospital No. 2. The operation of only TWO General Hospitals for the care of PW patients simplified both the administrative and security problems, and ultimately saved a number of US medical personnel. Enemy PW patients arriving at Ports of Debarkation, were transferred either to Glennan General Hospital or Camp Forrest General Hospital. Upon arrival they were sorted into 3 groups; convalescing patients were transferred to convalescent annexes; those requiring care for minor ills or injuries went to the nearby PW Station Hospitals; and those requiring more specialized treatment were kept at one of the 2 Prisoner of War General Hospitals. In addition, any PWs eligible for repatriation or for certification as “protected personnel” were held in special facilities at these Hospitals. Administration of the PW Hospitals consisted of duplicate staffs of US and German personnel. At the end of October 1944, the Army Chief of Staff directed ETOUSA Headquarters not to transfer any PW patients to the Zone of Interior, except rabid Nazis and those desired for questioning by Intelligence.
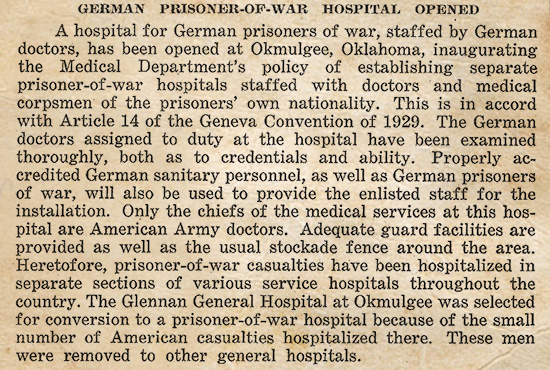
Copy of a 1944 local publication announcing the establishment of a German PW Hospital at Glennan General Hospital, Okmulgee, Oklahoma.
Following V-E Day, the repatriation of Prisoners of War program enabled to return Glennan General Hospital to the treatment of American patients in June 1945, to discontinue Camp Forrest General Hospital for treatment of enemy PWs and even to close subject camp in April 1946.
Port and Debarkation Hospitals:
Hospital installations were badly needed near Ports for the large numbers of transients: troops awaiting shipment overseas, or returning from overseas, as well as patients being returned to General Hospitals in the Zone of Interior for further treatment, and Port personnel. During 1942, and also in 1943, special Port Staging Area Hospitals were constructed for the care of transient troops and local personnel. These medical installations differed mainly from local Station Hospitals, because of their limited personnel and services, such as surgery, which was only set up to cope with possible emergencies.
Early February 1944, the existing practice whereby General Hospitals located near Ports of Embarkation / Debarkation were used as Receiving and Evacuation Hospitals was being reviewed by the Office of The Surgeon General. Throughout the later war years, the following Hospitals such as Halloran (Willowbrook, Staten Island) – Stark (Charleston, South Carolina) – and Letterman (San Francisco, California) General Hospitals continued to serve as Debarkation Hospitals, as the evacuation load grew heavier. At various times during the years 1944 and 1945, other General Hospitals including Lovell (Ayers, Massachusetts) – Barnes (Vancouver, Washington) – Birmingham (Van Nuys, California) – LaGarde (New Orleans, Louisiana) – Madigan (Tacoma, Washington) – McGuire (Richmond, Virginia) – and Mason (Brentwood, Long Island) served also in that way.
It must be stated that General Hospitals (in the ZI) accepted this role as Debarkation Hospital, reluctantly because the processing of patients in transit did not require full use of specialized equipment and staffs, and because hospitals engaged in Receiving and Evacuation had alternating periods of activity and idleness, depending upon the arrival of ships carrying patients! Some Officers agreed with Hospital Commanders that this process was wasteful to both personnel and equipment.
By end February 1944, The Surgeon General proposed the establishment of a new type of Hospital – designated Receiving and Evacuation Hospital – to be manned and equipped to perform ONLY the processing of patients in “transit”. The proposal was however not accepted and in April 1944, the existence of General and Station Hospitals for Debarkation purposes continued. Some units did however separate functions, with Stark – Letterman – and Halloran keeping apart their General Hospital functions from the specific debarkation work.
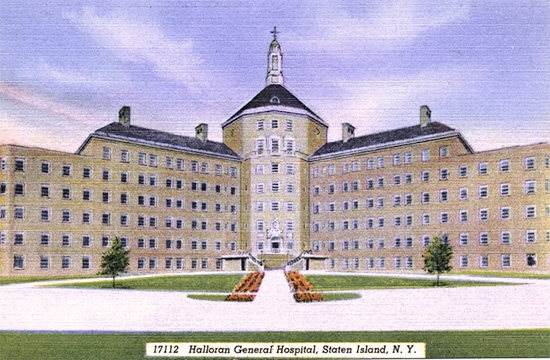
Vintage postcard illustrating Halloran General Hospital, Staten Island, New York.
As the need for beds in both General and Debarkation Hospitals increased, The Surgeon General secured approval of Army Service Forces Headquarters to use the Camp Edwards Station Hospital instead of the Lovell General Hospital as a Debarkation Hospital for Boston POE. Eventually an agreement was reached with the Chief of Transportation to convert certain hospitals in the Staging Areas of the Ports of Boston (Cp. Myles Standish), New York (Cp. Kilmer and Cp. Shanks), and Hampton Roads (Cp. Patrick Henry), to operate as Debarkation Hospitals. This allowed to free the McGuire and Camp Edwards General Hospitals, for specialized medical and surgical treatment. In addition to the above, the Camp Haan Regional Hospital was converted in 1945 to take over the further processing of debarking patients at the Los Angeles POE from Birmingham General Hospital.
Available Debarkation Hospital Beds
| Port / Hospital | October 1944 | March 1945 | June 1945 |
| Boston, Massachusetts | |||
| Camp Edwards Dbktn Hosp Boston POE |
2,128 | 800 1,700 |
900 1,700 |
| New York, New York | |||
| Halloran Dbktn Hosp | 2,799 | 2,700 | 2,700 |
| Kilmer Dbktn Hosp | 2,000 | 2,000 | |
| Shanks Dbktn Hosp | 2,300 | 2,300 | |
| Mason Dbktn Hosp | 1,000 | 500 | |
| Hampton Roads, Virginia | |||
| McGuire Dbktn Hosp | 1,577 | ||
| Patrick Henry Dbktn Hosp | 1,100 | 1,100 | |
| Charleston, South Carolina | |||
| Stark Dbktn Hosp | 2,162 | 2,125 | 2,400 |
| New Orleans, Louisiana | |||
| LaGarde Dbktn Hosp | 150 | ||
| Los Angeles, California | |||
| Birmingham Dbktn Hosp | 717 | 800 | |
| Camp Haan Dbktn Hosp | 800 | ||
| San Francisco, California | |||
| Letterman Dbktn Hosp | 2,000 | 3,140 | 3,140 |
| Seattle, Washington | |||
| Madigan Dbktn Hosp | 500 | 1,000 | 1,000 |
As the evacuation of patients by air increased during 1944 and 1945, the Army Air Forces selected certain Station and Regional Hospitals located near important Fields to receive and process patients returning to the Zone of Interior. In total eleven (11) AAF Hospitals were reserved for this purpose, including such places like Mitchel Field (New York), Coral Gables (Florida), Hamilton Field (California), Great Falls (Montana), and Portland (Oregon).
WAAC / WAC Hospitals:
Certain Army Hospitals held ‘special’ wards reserved for hospitalization of service women. The expansion of female volunteers in May 1942, destined for the WAAC (or later WAC), and other Branches and Services, called for procurement of limited numbers of female physicians, contract surgeons, and commissioned staff to serve in hospitals where the WAAC (or other) patient load was expected to be high. As a result 3 Army Hospitals were chiefly occupied by female patients; they were Ft. Des Moines, Iowa – Ft. Oglethorpe, Georgia – and Daytona Beach, Florida, all located near or at WAAC Training Centers.
In May 1943, the Surgeon General assigned a woman Medical Corps Officer to his Office to supervise the handling of medical problems peculiar to female personnel.
Equipment Lists
Equipment Lists for Hospitals and other Medical Units
Army Service Forces Catalog MED 10 – Headquarters, Army Service Forces – 1 March 1944, Medical Supply Catalog: MED 10-5 – Hospital Trains
Item 9738200 – Kitchen-Dining-Pharmacy Car, Communications Zone, Medical Equipment
Item 9738300 – Officer’s Personnel Car, Commmunications Zone, Medical Equipment
Item 9738400 – Orderly Car, Commmunications Zone, Medical Equipment
Item 9738500 – Unit Car, Zone of Interior, Medical Equipment
Item 9738600 – Utility Car, Communications Zone, Medical Equipment
Item 9738700 – Ward Car, Zone of Interior, Medical Equipment
Item 9738800 – Ward Car, Communications Zone, Medical Equipment
Item 9738900 – Ward Car, Modified, Zone of Interior, Medical Equipment
Item 9739000 – Kitchen Car, Zone of Interior, Medical Equipment (introduced 15 Oct 43)
Equipment Lists for Hospitals and other Medical Units
Army Service Forces Catalog MED 10 – Headquarters, Army Service Forces – 1 March 1944, Medical Supply Catalog: MED 10-4 – Ship Medical Equipment
Item 9720100 – Ambulance Ship, Medical Equipment
Item 9723905 – Hospital Ship, Medical Equipment, 200-Bed (introduced 15 Oct 43)
Item 9723910 – Hospital Ship, Medical Equipment, 500-Bed (introduced 15 Oct 43)
Item 9723915 – Hospital Ship, Medical Equipment, 1000-Bed (introduced 15 Oct 43)
Item 9723920 – Hospital Ship, 100-Bed Expansion Unit (introduced 15 Oct 43)
Item 9733050 – Transport, Medical Equipment
Item 9733055 – Transport, Medical Expansion Unit
Equipment Lists for Hospitals, Communications Zone
Army Service Forces Catalog MED 10 – Headquarters, Army Service Forces – 1 March 1944, Medical Supply Catalog: MED 10-2 – Communications Zone Hospitals
Item 9723500 – General Hospital, Communications Zone, 1000-Bed
Item 9723600 – General Hospital, Communications Zone, 1500-Bed (introduced 10 Feb 44)
Item 9723700 – General Hospital, Communications Zone, 500-Bed (introduced 10 Feb 44)
Item 9723800 – General Hospital, Communications Zone, 200-Bed
Item 9724700 – Hospital Expansion Unit, Communications Zone, 25-Bed
Item 9724900 – Hospital Expansion Unit, Communications Zone, 50-Bed
Item 9725100 – Hospital Expansion Unit, Communications Zone, 100-Bed
Item 9725300 – Hospital Expansion Unit, Communications Zone, 250-Bed
Item 9725500 – Hospital Expansion Unit, Communications Zone, 500-Bed
Item 9731000 – Station Hospital, Communications Zone, 25-Bed
Item 9731200 – Station Hospital, Communications Zone, 50-Bed
Item 9731500 – Station Hospital, Communications Zone, 100-Bed
Item 9732000 – Station Hospital, Communications Zone, 250-Bed
Item 9732300 – Station Hospital, Communications Zone, 500-Bed
Item 9732500 – Station Hospital, Communications Zone, 750-Bed
Medical Supply Catalog: MED 10-3 – Miscellaneous Communications Zone Units
Item 9721000 – Convalescent Camp, 1000-Bed
Item 9722700 – Field Hospital, 400-Bed (Field Hospitalization Unit > Item 9722705)
Item 9723005 – General Dispensary Equipment, Type I, Communications Zone
Item 9723010 – General Dispensary Equipment, Type II, Communications Zone
Item 9725700 – Infirmary Equipment, Communications Zone, 10-Bed
Medical Supply Catalog: MED 10-16 – Individual Equipment List
Item 9722500 – Evacuation Hospital, 750-Bed
Medical Supply Catalog: MED 10-17 – Individual Equipment List
Item 9722300 – Evacuation Hospital, Semimobile, 400-Bed
Medical Supply Catalog: MED 10-18 – Individual Equipment List
Item 9729300 – Portable Surgical Hospital, Communications Zone, 25-Patient (introduced 15 Jun 44)
Equipment for Hospitals, Zone of Interior
Army Service Forces Catalog MED 10 – Headquarters, Army Service Forces – 1 March 1944, Medical Supply Catalog: MED 10-7 – Zone of Interior Hospitals
Item 9724600 – Hospital Expansion Unit, Cantonment Type, Zone of Interior, 25-Bed
Item 9724800 – Hospital Expansion Unit, Cantonment Type, Zone of Interior, 50-Bed
Item 9725000 – Hospital Expansion Unit, Cantonment Type, Zone of Interior, 100-Bed
Item 9725200 – Hospital Expansion Unit, Cantonment Type, Zone of Interior, 250-Bed
Item 9725400 – Hospital Expansion Unit, Cantonment Type, Zone of interior, 500-Bed
Item 9730900 – Station Hospital, Cantonment Type, Zone of Interior, 25-Bed
Item 9731100 – Station Hospital, Cantonment Type, Zone of Interior, 50-Bed
Item 9731300 – Station Hospital, Cantonment Type, Zone of Interior, 100-Bed
Item 9731700 – Station Hospital, Cantonment Type, Zone of Interior, 250-Bed
Item 9732100 – Station Hospital, Cantonment Type, Zone of Interior, 500-Bed
Item 9732400 – Station Hospital, Cantonment Type, Zone of Interior, 750-Bed
Item 9723400 – Station Hospital, Cantonment Type, Zone of Interior, 1000-Bed

Overview of the Tripler General Hospital in Honolulu, Hawaii.
Equipment for Operating Teams
Army Service Forces Catalog MED 10 – Headquarters, Army Service Forces – 1 March 1944, Medical Supply Catalog: MED 10-15 – Operating Teams
Item 9720300 – Auxiliary Surgical Group, Equipment
Item 9733005 – Team, Gas (introduced 15 May 44)
Item 9733006 – Team, General Surgical (introduced 15 May 44)
Item 9733008 – Team, Maxillo-Facial (introduced 15 May 44)
Item 9733009 – Team, Neurosurgical (introduced 15 May 44)
Item 9733010 – Team, Orthopedic (introduced 15 May 44)
Item 9733012 – Team, Shock (introduced 15 May 44)
Item 9733014 – Team, Thoracic Surgery (introduced 15 May 44)
Item 9959110 – Truck, 2 ½-Ton, 6 x 6, Surgical, Operating, Medical Equipment For (introduced 15 May 44)
Note: A new Medical Department Equipment List, superseding existing or tentative lists, dated 1 November 1944 was distributed with Army Service Forces Catalog MED 10-5 with following entries:
Item 9720300 – Auxiliary Surgical Group, Equipment
Item 9733001 – Team, Blood Transfusion, Type I (Small)
Item 9733002 – Team, Blood Transfusion, Type II (Large)
Item 9733005 – Team, Gas
Item 9733006 – Team, General Surgical
Item 9733008 – Team, Maxillo-Facial
Item 9733009 – Team, Neurosurgical
Item 9733010 – Team, Orthopedic
Item 9733012 – Team, Shock
Item 9733014 – Team, Thoracic Surgery
Item 9733040 – Team, X-Ray
Item 9959110 – Truck, 2 ½-Ton, 6 x 6, Surgical, Operating, Medical Equipment For