Brief Overview of the Medical Department

Medical personnel of the 104th Infantry Division examine the remains of one of their 3/4-ton Weapon Carriers hit by an enemy artillery shell in Arnoldsweiler, Germany, 25 February 1945.
This article has been produced to offer a brief overview of the Medical Department during the Second World War. Many of the features which are included in this article can be found in more detailed articles referring exclusively to that subject.
For more detailed information regarding the Identification of Medical Personnel, please click here.
Background Information:
The United States Army Medical Department and the Medical Corps trace their origins to 27 July 1775, when the Continental Congress established the first Army Hospital. Congress also provided a medical organization of the Army only in time of war or emergency until 1818, which marked the inception of a permanent and continuous Medical Department.
There were THREE different aspects of the Army medical problem:
| FIRST | Selection of those upon whom the security of the nation depends, to be sure they are physically fit to endure the rigors of warfare. |
| SECOND | Preservation of the health of the able bodied in the military service. |
| THIRD | Restoration of the health of those who become sick or injured. |
The principal service functions of the Medical Department were:
- Evacuation
- Hospitalization
- Sanitation
- Procurement, Storage and Issue of medical supplies.
The Medical Department was charged with care of sick and wounded men and animals (still used during WW2) and transportation necessary for their evacuation and hospitalization; prevention of disease, including direction and supervision of measures of public health among inhabitants of occupied territory; sanitation, including inspection of meats, foods, and dairy products; and preparation and proper disposition of medical records.
The Corps of the Medical Department:
The Medical Department was organized into the Medical Corps, the Dental Corps, established in 1911, the Veterinary Corps, established in 1916, the Medical Administrative Corps, established in 1917, the Sanitary Corps, also established in 1917, and the Army Nurse Corps, established in 1901. Additional Departments were introduced in 1942, such as the Hospital Dietitian Corps, the Physical Therapist Corps, and the Pharmacy Corps, which followed in 1943. Civilian doctors joined the Department as ‘Contract Surgeons’, while the Army equally started accepting female doctors. A Medical Reserve Corps was already established in 1908.
| Insignia of the Medical Department | ||
|---|---|---|
 |
 |
 |
| Insignia of the Medical Corps |
Insignia of the Dental Corps |
Insignia of the Veterinary Corps |
 |
 |
 |
| Insignia of the Army Nurse Corps |
Insignia of the Sanitary Corps |
Insignia of the Medical Administrative Corps |
 |
 |
 |
| Insignia of a Contract Surgeon |
Insignia of the Hospital Dietitian Corps |
Insignia of the Pharmacist Corps |
 |
||
| Insignia of the Physical Therapist Corps |
||
| © 2007 WW2 US Medical Research Centre www.med-dept.com |
||
The Caduceus became the only official collar ornamention on uniforms, and was widely applied on equipment too (the former Maltese Cross was discarded). Maroon became the new Medical Department’s official color (replacing green).
The medical symbol, i.e. the Caduceus (1” high) was approved in 1902 only (although already designed in 1851), and the different branch insignia used a gold color metal Caduceus, with a superimposed brown (early) and/or black (late) enamel capital letter indicative of their respective Corps.
The Medical Department
The Medical Department is the service of the Army that maintains its health, treats its sick, and heals its wounded. Through physical examination, the Medical Department selected for admission to the Army of the United States only those who were in good physical condition. It kept Army personnel in good physical shape through periodic examinations for the purpose of discovering any defects early, so that prompt steps could be taken to remedy them and to always keep the Army’s fitness for National Defense at high level.Every activity of the soldier in every hour of every day, in peace and in war, was of concern to the Medical Department. Army Medical Officers watched to see that the G.I.’s surroundings were as healthful as the conditions under which he was to perform his duties. They advised all commanders of suitable measures to preserve health and prevent and control disease.Continuous service of the Medical Department was given to the Armed Forces personnel through a series of medical installations, ranging from the unit Dispensary where mild cases were treated to the large General Hospitals at which serious cases were diagnosed and handled. In time of peace, the doughboy was treated in permanent Hospitals conveniently located to his place of duty, and mainly in the Zone of Interior. In war, mobile medical units did their work on and near the battlefields and combat zones to bring back the wounded, give them treatment in Aid Stations and mobile Hospitals, and move them to General Hospitals in the rear.
In 1939, on the eve of World War 2, the Medical Department consisted of the Surgeon General (with rank of Major General), of four Assistant Surgeon Generals (with rank of Brigadier General), one from the Dental Corps, five separate Corps of Officers and Enlisted Men (later to be expanded), and a number of civilian employees. The Surgeon General was also the Medical Adviser to the Secretary of War and the Chief of Staff.
Total strength of the Medical Department, on 30 June 1939, was only 27,139 Officers and 21,279 EM (as opposed to a total WW1 peak of 340,000 men).
The different Corps of the Medical Department formed independent branches with following responsibilities:
The Medical Corps extended about 7,500,000 treatments and cared for approximately 270,000 patients in Hospitals during each year in time of peace. Patients included not only Army personnel, but also Veterans’ Administration (VA) and Civilian Conservation Corps (CCC) patients. Officers also held many duties other than those which were purely professional. Medical supply, sanitation, command structure of Hospitals, command of mobile medical units, and instruction in Medical Department Service Schools, and service to other arms and services were the more important of these duties. This branch of the Medical Department gave medical and surgical treatment, but NO dental treatment.
The Dental Corps provided dental care to the Army, and made periodic inspections to discover the need for dental treatment. Over 250,000 treatments were given each year.
The Veterinary Corps took care of military animals and regularly inspected food and forage used by the Army. Officers of this Corps commanded the veterinary units of the Army both in peace and in war. Vets treated sick and wounded animals, but also supervised dairies, inspected refrigeration and storage plants, meat and dairy products, and performed other similar duties. The Officers were qualified Veterinarians.
The Officers of the Medical Administrative Corps helped conduct the work of the Medical Department at the larger Hospitals and Headquarters, where they performed administrative duties. They consisted largely of WW1 Officers with administrative experience who had continued serving in the Reserves after the war.
The Sanitary Corps was established in time of war to supervise and regulate the sanitation of places occupied by the Military Forces. This also included work in certain aspects of the field of preventive medicine, since most men already had some experience and college training in technical fields allied to medicine (such as chemistry, sanitary engineering, hospital architecture).
The Army Nurse Corps gave assistance in the care of sick and wounded. Their members had relative rank from Second Lieutenant to Major, and were on duty at about 40 different General and Post Hospitals in the United States and at overseas stations. In time of war many additional Nurses would come from Schools or were obtained through the American Red Cross.
Hospital Dietitians were female members of the Medical Department who planned and supervised meals in Army Hospitals. They were equivalent in rank to an Officer, and were usually Second Lieutenants.
Physical Therapists were also female members of the Medical Department. They were trained in the use of physical exercises as a treatment for certain diseases and physical defects. They could hold either a Commissioned or an Enlisted grade.
The Pharmacy Corps was the branch that was made up of Regular Army Officers who were graduate Pharmacists, and of all Regular Army Officers who were formerly in the Medical Administrative Corps. Their major task was being responsible for matters of administration and pharmaceutics that concerned the Medical Department.
Contract Surgeons were civilian physicians who performed professional and administrative functions of a Medical Officer, but without military rank or Commission (changes were to take place later in WW2).
The Medical Department maintained a fair number of completely equipped and fully staffed General Hospitals, and Hospitals of smaller sizes at most Army Posts. Active Medical Battalions were assigned to the different Army Divisions. Medical equipment and supplies were obtained, stored, and issued from Medical Supply Depots operated by the Medical Department. The Department devised and tested equipment to assist in the care of patients, such as First-Aid Kits and Packets, Litters, Ambulances, and motorized field equipment as well as surgical operating facilities. Vaccines for the prevention and treatment of certain diseases, and other laboratory products, were equally prepared in the laboratories of the Army Medical School in Washington. The Army Medical Library (Washington D.C.) was the largest in the world for it stored over 1,000,000 books and manuscripts.
The Army Surgeon General was a member of the Central Committee of the American Red Cross and advised that organization on the assistance it could give in time of war. The Medical Department furnished medical personnel, mobile units, and supplies, to assist civil agencies in times of disaster, and cooperated with the A. R. C. in such work. In addition the Department provided complete medical service for the Civilian Conservation Corps, utilizing therefore Regular Army medical personnel and some 1,400 Reserve Officers (of the M.D.). It examined all enrolees, gave them protective inoculations against diseases, supervised general sanitation, inspected food and water, furnished necessary medical supplies, and cared for the sick and wounded.
The outbreak of WW2 and the continuous military build-up, escalating into full mobilization, would transform the Medical Department along with the rest of the United States Army. In the months before the Japanese attack against Pearl Harbor, medical strength grew to 131,586 Officers and Enlisted Men, a rate of increase, even more rapid than that of the Army as a whole. It would further expand during the war…
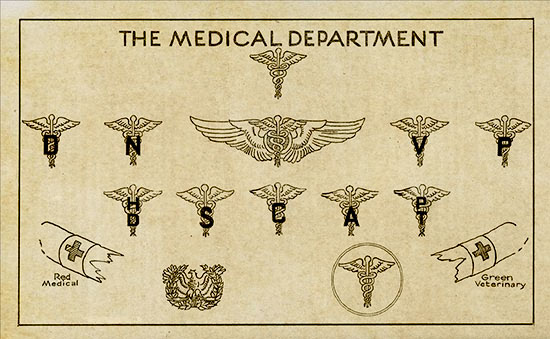
1944 Chart illustrating the different US Army Medical Department Branch Organizations Insignia.
Branch Colors & Guidons:
Medical Detachment:
Tables of Organization provide for each Regiment and separate Battalion of every arm and service (except Medical), a group of medical troops. The term “attached” applies to these Detachments. By definition, both a Battalion and a Regiment are units composed organically of the troops of a single arm or service. For this reason, any component of a Battalion or a Regiment made up of troops of another arm or service (i.e. in this particular case, medical troops), must be attached, rather than assigned. The Medical Detachment, which is the foundation upon which is erected the entire structure of field medical service (first echelon), occupies the same relative position in the unit (it serves), as a Company, Battery, or Troop. The Regimental Surgeon is not only a Staff officer of the Regimental Commander, he is also in direct command of the Regimental Medical Detachment. In the Infantry Division, there are 6 Medical Detachments, one for each of the three Infantry Regiments, one for the Division Artillery, one for the Engineer Combat Battalion, and one for all remaining division troops, including Special Troops. Each of the three Infantry Regimental Medical Detachments consist of one Headquarters Section and three Battalion Sections (which provide medical support for one of the three Infantry Battalions in the Regiment):
Medical Detachments in the Infantry Division.
Typical branch colors were maroon piped with white, already specified in October 1916. This piping was often worn on the garrison cap (or overseas caps) of Enlisted Men, while Medical Officers retained the standardized black/gold piping indicating commissioned personnel. Attached medical personnel (members of the Medical Detachment) retained identical clothing as the infantrymen, adding the specific medical supplies and individual gear necessary to the service. Only branch insignia and piping could identify the aidmen; they wore the Medical maroon/white piping on their headdress instead of the Infantry light blue, and the Medical Caduceus replaced the Infantry crossed muskets on the collar disks. Being attached to the Infantry Regiment, they were considered to be part of this organization, and as such medical personnel displayed the enamelled Regimental Distinctive Insignia (D.I.) on both lapels of the service jacket and the garrison cap (for E.M.) and on the shoulder loops of the service coat (for Officers). Unit identification, or Guidon, in the form of a swallow-tailed flag without fringe attached to a flagstaff, below the spearhead, represented both color and distinguishing marks of the organization. The standard bearer of the attached Medical Detachment used a Guidon similar to that of the main Infantry group, i.e. a dark blue Guidon, with the Regiment’s number high up, the Infantry crossed muskets in the center, and the block letters MED in the lower part, all in white bunting:

Guidon of the Medical Detachment, 395th Infantry Regiment, 99th Infantry Division, Campaigns: Rhineland, Ardennes-Alsace, Central Europe
Medical Battalion:
The Medical Battalion is one of the organic (i.e. not attached) Battalions that is part of the Infantry Division (also Armored and Mountain Divisions included such units, while the Cavalry Division had a Medical Squadron, and the Airborne Division ran an organic Medical Company) or other similar organizations which perform second echelon medical service for the Division. It consists of one Battalion Headquarters and Headquarters Detachment, three Collecting Companies, and one Clearing Company. Each of the three identical Collecting Companies is an autonomous element of the Battalion designed to provide medical support for one of the three Regiments (or Combat Teams) of the Division, including evacuation of casualties from Aid Stations, their treatment in Collecting Stations, and finally, evacuation to the Division Clearing Station. The Collecting Company evacuates all units within the zone of action of its respective Infantry Regiment.The Clearing Company operates one or two Clearing Stations near the Division rear boundary for the further care and treatment of casualties, pending their removal from the Division area by third echelon (Army) medical service. The senior available Officer of the Medical Corps is the Battalion Surgeon:

Illustration of a typical Medical Unit Guidon (Replacement Training Center, Regiment, Battalion). Std. colors are maroon (background) and white (Caduceus). This is an example of an unassigned Guidon, i.e. neither numbers nor letters have yet been added.
Organization of the Medical Battalion.
Typical branch colors were of course medical maroon piped with white, as used by the Medical Detachment. Same rules for uniform ornamentation also applied here. Medical personnel wore the specific individual equipment and gear as used by their parent organization (be it Infantry, Armor, Cavalry, Airborne). Being an organic unit, branch insignia and piping remained medical, and contrary to the Medical Detachment (see above), its members displayed the enamelled Medical Battalion Distinctive Insignia (D.I.) on garrison caps, service coat lapels, and shoulder loops. Another difference with the Medical Detachment was the Guidon – this was one bearing the medical colors, i.e. a maroon field, with the Battalion’s number high up, the Medical Caduceus in the center, and block letters indicating the Company in the lower field, all in white bunting:
Guidon of B Company,
2d Medical Battalion, 2d Infantry Division,
Campaigns: Normandy, Northern France, Rhineland, Ardennes-Alsace, Central Europe
Medical Vehicle Markings:
Medical Detachment:
Likewise, markings for the vehicles operated by the Medical Detachment reflected the Infantry Regiment to which they were attached. Unit identification symbols (front and rear of vehicle) consisted of four groups arranged in consecutive order, from L to R, when facing the vehicle. The first group illustrated the highest hierarchic unit (here, 26th Inf Div), followed by the second group designating the Regiment (here 104th Inf Regt). The third group, designating the lesser component (Company or similar organization, here, Med Det) covered the latter part of the bumper, together with the fourth group, indicating the serial number of the vehicle (here, 3). Identical groups were to be respected for the bumperettes. Standard dimensions were 3 inch high (front bumper) and 2 inch high symbols in fractions (rear bumperettes), applied with white gasoline solvent paint, either with the help of stencils, or simply by hand:
Explanation: from L to R – 26th Infantry Division, hyphen, 104th Infantry Regiment, hyphen, Infantry symbol, small 3-in star, Medical Detachment symbol, hyphen, 3d vehicle.
Functional Organization of the Medical Detachment, Infantry Division
Medical Battalion:
Vehicles naturally reflected the Division to which the Medical Battalion pertained, Infantry, Armor, Cavalry, or Airborne. Unit identification symbols were applied as per Army regulations (A.R.) and consisted of the standardized four groups of symbols, arranged in consecutive order, from L to R, when facing the vehicle. In this particular case, the markings represented some of the subunits comprising the Battalion. Dimensions and paint were standard applications.

Explanation: from L to R > 5th Armored Division, Armored symbol, 75th Armored Medical Battalion, Medical symbol, small 3-inch star, Collecting Company, hyphen, 2d vehicle.
Organization of a Collecting Company.
Remark: for more detailed information about Medical Vehicle Markings, please click here to view extra texts on the subject. For extra data related to the Identification of Medical Personnel in the field, please click here.
The Make Up of the Medical Field Units:
In a Division, the Medical Department provides two main echelons of medical service for the care and evacuation of casualties from forward areas. The first echelon consists of the Medical Detachment, and the second echelon is the Medical Battalion.
The Medical Detachment accompanies the unit to which it is attached in all tactical operations, and functions under the immediate control of the unit’s commander. Its strength, organization, and operation vary according to the unit to which it is attached (Infantry, Armor, Mountain, Cavalry, Airborne). The tactical employment of such medical unit is thus governed by the special characteristics of the arm or service to which the Medical Detachment belongs. The variations in field situations and combat methods require appropriate modifications of the internal organization of the Sections of unit Medical Detachments. Once more, the importance of the functions of Medical Detachments cannot be overemphasized, for their personnel are the first medical men to reach a casualty. Their emergency medical treatment, rendered on the spot and frequently under fire, often means the difference between life or death for the wounded. They therefore are the keystone for the entire medical evacuation system!

Schematics illustrating First Echelon Medical Service
Brief Organization:
Medical Detachment, Infantry Regiment – each of the three Infantry Regimental Medical Detachments consists of one Headquarters Section and three Infantry Battalion Sections. Their functions and areas of activity cover medical service rendered in garrison, on the march, and in combat; furthermore, they are responsible for equipment, transportation, training, administration, and supply. The characteristics that influence the Medical Detachment are as follows: the Infantry Battalion is the basic tactical unit, operating over relatively large areas, and occupying frontages varying between 500 and 3,000 yards. Infantry is exposed to fire of all types of weapons and to air action. The casualty rate of Infantry is higher than any other arm or service. Infantry must be able to maneuver and to fight over all kinds of terrain.
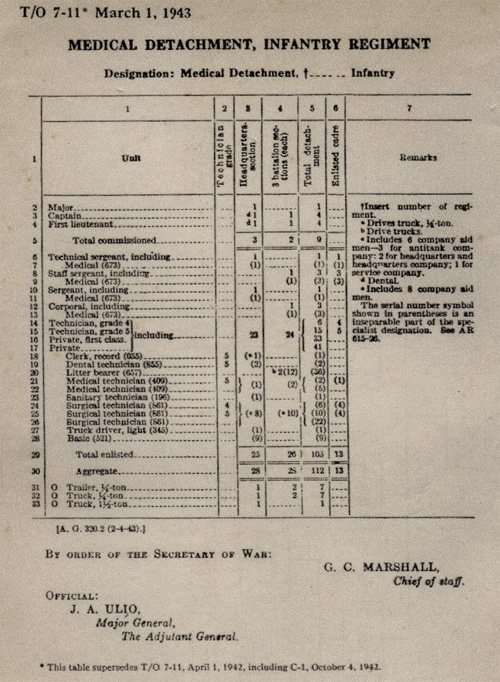
Table of Organization, T/O 7-11 dated 1 March 1943, illustrating the Medical Detachment of an Infantry Regiment
Medical Detachment, Division Artillery – consists of one Headquarters Detachment and four Battalion Detachments. The five units normally operate independently of each other. Their task is to give medical support to the Headquarters and Headquarters Battery, and the four identical Battalions, i.e. three 105-mm Howitzer Battalions, and one 155-mm Howitzer Battalion. Artillery Battalions are the basic tactical units. When they are part of a large Artillery force, the area assigned is relatively small, and within the Battalion area, the Batteries are usually echeloned only sufficiently to avoid too compact a target. The characteristics that influence the Medical Detachment are as follows: Artillery units are rarely exposed to small arms fire, consequently, their casualty rate is less than that of the Infantry, and they tend to occur at irregular intervals. A Battalion position is a relatively fixed arrangement, and Artillery does not maneuver when actually engaged. The majority of Artillery positions are often farther to the rear.

Aid Man escorting 2 Casualties to the Rear
Medical Detachment, Engineer Combat Battalion – consists of two main functional groups, the Company Aid Squad, and the Aid Station Squad. The characteristics that influence the Medical Detachment are as follows: the Engineer Battalion is frequently dispersed in the Division area, and even Companies and Platoons are often separated. In a combat situation, the small size of the Medical Detachment often requires the scattered Engineer elements to obtain incidental medical service from other units in the vicinity. Because of this situation, reinforcement is often necessary, particularly with litter bearers (temporarily drawn from the ranks of the Engineer unit). As the limited number of aid men cannot be attached on the basis of one per Platoon, they must be attached according to the size of the unit, the circumstances, and the distance at which the unit is operating from the Aid Station.
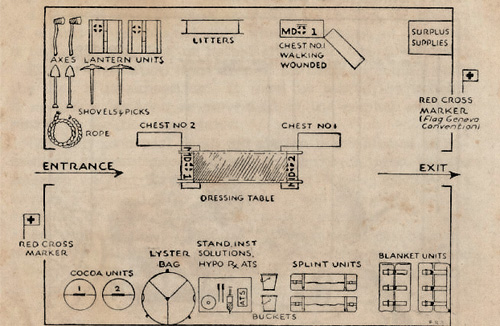
Arrangement of a typical Aid Station
Medical Detachment, Special Troops – consists of a limited number of medical troops for the Signal Company, and the three Reconnaissance Platoons. The remainder of the Medical Detachment will establish and operate an Aid Station in the vicinity of the rear echelon of Division Headquarters, to provide medical service to the other troops, such as the Headquarters Company, the Military Police Platoon, the Ordnance Company, and the Quartermaster Company.
Typical Equipment of a Battalion Medical Section
Other Medical Detachments are those attached to and supporting Armored Divisions, Mountain Divisions, Cavalry Divisions, and Airborne Divisions. Also non-Divisional units, such as Tank Destroyer Battalions, Antiaircraft Artillery Battalions, Quartermaster and Signal Battalions have small Medical Detachments. In fact, every unit the size of a Battalion (or larger) has a Medical Detachment.
The Medical Battalion is the organic unit of the Division, performing field medical service for the entire Division. It consists of one Battalion Headquarters and Headquarters Detachment, three Collecting Companies, and one Clearing Company. The various functions include equipment, transportation, training, administration, supply, maintenance, messing, and general care of sick and injured.
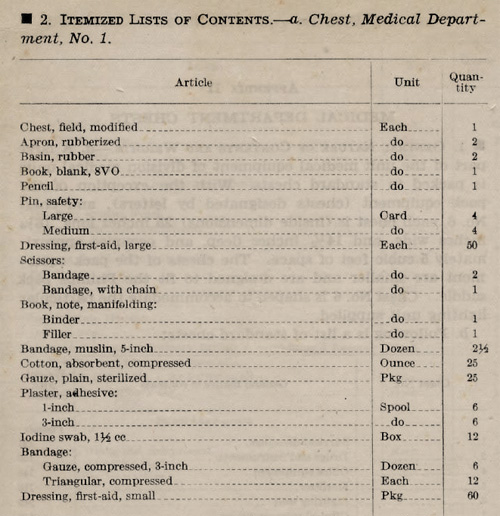
Itemized List of Contents of a Medical Department Chest No. 1
Brief Organization:
Headquarters and Headquarters Detachment – main functions are command and staff operations, personnel administration for all units, requisition and procurement of medical supplies for the entire Division, and of all classes of supply for the Battalion itself, and second echelon motor maintenance for all Battalion vehicles. In view of these functions and activities, the Hq and Hq Det will also operate, a Division Medical Supply Point, a Battalion Supply Point, and a Battalion Motor Repair Park. Due to its different number of functions, it is divided into Sections, i.e. Detachment Headquarters – Personnel – General and Medical Supply – Motor Maintenance. The Detachment is an autonomous part of the Medical Battalion (comparable to the other four Companies) and directly subordinate to the Battalion commander.

Medic administering First Aid to a Wounded Soldier
Collecting Company – each of the three identical Collecting Companies is an autonomous element within the Medical Battalion, designed to give medical support to an Infantry Regiment. It consists of one Company Headquarters and three Platoons. The latter represent Station Platoon – Litter Bearer Platoon – Ambulance Platoon (and sometimes an improvised Liaison Section). Main functions cover evacuation of casualties from the Aid Stations operated by the Infantry Regiment Medical Detachment (usually performed by litter), maintaining contact with the Aid Stations (with help of a Liaison Section), and operating a Collecting Station for casualties requiring treatment while en route to the rear. Further they are responsible for evacuating casualties from the Collecting Station to the Division Clearing Station (use of an Ambulance Shuttle is therefore mandatory), and for replenishing medical supplies of Aid stations (combat support). Other important activities are command, administration, supply, mess, and motor maintenance.
Schematics illustrating a Collecting Station

Form of typical Directing Sign for a Collecting Station
Clearing Company – consists of one Company Headquarters and two identical Clearing Platoons, each capable of operating independently a Clearing Station. Its main function is to operate the Clearing Station for treatment of all casualties suffered in the Division. These activities include reception, sorting, providing temporary care and shelter, and returning the slightly injured to duty with their unit. The functions of a Clearing Company are largely technical and of professional nature, only a small amount of administrative work is necessary (mainly preparation of appropriate medical records).
Set Up of a typical Clearing Station
It should be noted that the organization and employment of medical troops pertaining to Cavalry, Mechanized or Armored Divisions, and ‘special’ units such as Mountain Divisions or Airborne Divisions, always reflect the large parent unit characteristics in the field and in combat.

“Bill Mauldin’s Army”, by Bill MAULDIN, Presidio Press, Novato, California, 1984
(Cartoon drawn by Sgt W. Mauldin 1921-2003)
The Hague & Geneva Conventions:
“If you should be CAPTURED – these are your rights”Booklet to inform US Army personnel about their rights as a prisoner of war and major data governing the Geneva Convention Relative to the Treatment of Prisoners of War, War Department Pamphlet No. 21-7, Washington 25, D.C., 16 May 1944
“The Hague Convention”, (last one held in 1907), was held in order to consider, among other things, the treatment of prisoners of war and of inhabitants of occupied territory. Non-belligerents were prohibited from engaging in combat and in other forms of direct action against the enemy, except in self-defense. If they violated this law of war and were captured by the enemy, they were NOT entitled to the protection guaranteed prisoners of war, and could be punished! These laws of war were therefore included in The Hague Conventions. “The Geneva Convention” (of 1929) indicated the obligations of all belligerents to respect the sick and wounded, without distinction of nationality. It was also their duty to search, care and protect the wounded, and to arrange for burial or cremation, and to make every effort to record the identity of dead enemies. Medical troops, installations and equipment were to be protected so long as they would not be used to commit acts injurious to the enemy (this protection was also extended to dental corps personnel, but NOT to the veterinary service). The medical service emblem (Red Cross or Geneva Cross) was to be displayed on all flags, brassards, equipment (if feasable), used by the medical service. This emblem could not be used by any other branch of the military service!
WW2 Medical Department Statistics and Figures:
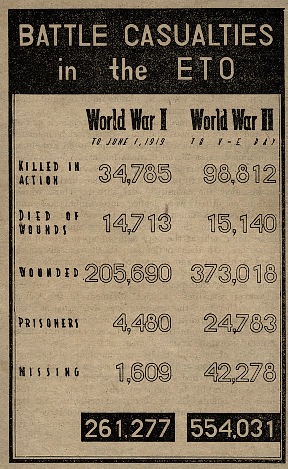
Wartime chart showing the comparison between battle casualties of World War 1 and WW2 in the ETO”American Enterprise in Europe – The Rôle of the SOS in the defeat of Germany”.
Printed by Chief Information & Education Division, USFET, Paris, France, June 1945
In WW2, efficient medical care reduced overall losses to only 4 in each 100 wounded (WW1 8 out of 100). Better surgery, penicillin, plasma and whole blood were responsible in varying degrees, however the credit must be shared by the entire personnel of the Medical Department, whose painstaking care, surgical skill and devotion to duty under difficult and dangerous conditions saved thousands of lives! The soldier with an infection of his wounded leg, or with an open chest wound, or a mutilated face, or an injured brain, was certain to receive, after a short interval, the care of an orthopedic, plastic or neuro-surgeon – until he could reach his specialist. In general, the G.I. received the type of care which would get him to that specialist in the best possible condition. Army Nurses also gave widely varying types of skilled and sympathetic (often called Angels) service, some in field hospitals and others in general hospitals farther back. WW2 was also the first war in which Nurses automatically held officer rank! (in May 1945 there were 17,314 active Nurses in the ETO).
Prior to D-Day, June 1944 ETO medical personnel totaled 132,705, of whom 62,000 were with combat forces and the rest with the Services of Supply (S.O.S.) – by March 1945 the number had increased to 245,387 men. During WW2 the Medical Department’s field forces totaled 13,174 casualties, of which 2,274 were killed. Overall battle casualties in the ETO were as follows: 554,031 men & women (up to V-E Day). This can be subdivided into KIA = 98,812, WIA = 373,018, MIA = 42,278, POW = 24,783, died of wounds = 15,140. The percentage among arms and services was split into Infantry = 75.02%, Air Forces = 9.36%, Artillery = 5.40%, Corps of Engineers = 3.03%, Medical Department = 2.47%, Armored Forces = 1.01%, and others = 3.71%. Also, deaths from disease in WW1 were more than 31 times greater than those suffered in WW2, while lost service due to venereal disease (V.D.) was 30 times higher in WW1 than during WW2 … (although WW2 still numbered 606 men who came down with VD each day).